Treatment Readiness: Clinical workflow strategy and decision support for oncology operations
UX Research & Design Strategy Lead
Designing for the preparation work behind treatment readiness.
A 2-minute ordering action became clearer when we mapped the hours of clinical, inventory, and EHR coordination that made it possible. Through customer research, workflow mapping, and concept validation, I reframed a legacy dispense queue into a readiness-driven workflow for oncology operations.
The coordination work was already happening — across people, systems, and timing. The design opportunity was to bring it into the platform.
From transaction to readiness.
Before, the queue treated dispensing as a transaction: patient, drug, quantity, action. After, the workflow treated dispensing as an operational readiness problem: appointment timing, clinical status, EHR dependencies, inventory availability, exceptions, and human review.
Treatment readiness depended on a coordinated workflow across people, systems, and timing.
Teams were checking schedules, reviewing clinical context, confirming inventory, watching for EHR updates, and resolving exceptions before a dispense action could happen. Most of that work was invisible to the platform.
The visible action was simple. The work behind it was not.
One participant spent 4 hours every morning building the queue patient by patient — searching, confirming drug and dose history, checking the EHR in a second window, calculating vials manually, then queueing. The 2-minute dispense action at the end of the day was the product's visible surface. The preparation work that made it safe was invisible to the system entirely.
The preparation work that happened before, around, and outside Lynx.
Three participants across Rheumatology/NextGen, Oncology/Varian, and Oncology/iKnowMed G2 contexts.
The readiness workflow crossed clinical, pharmacy, inventory, billing, and EHR dependencies before a dispense action could happen. Most of it was invisible to the platform.
Four decisions that shaped the workflow direction.
Make readiness visible before action
Surface who is ready for dispense, who is blocked, and what is missing — automatically, before the patient arrives. No manual queue construction.
Separate blocked work from ready work
The Queue was acting as planning tool, readiness monitor, and execution list at once. Separate those jobs into clearer workflow moments with distinct information needs.
Show why something is blocked, not just that it is
Dose changes, EHR validation gaps, and inventory shortfalls are expected states. Users need to understand what changed and what they can do about it — not just that there's a problem.
Support override with context and accountability
The system carries calculations and recommendations. Humans retain review, adjustment, and approval before any ordering or dispense action is taken.
Built to validate direction before engineering commitment.
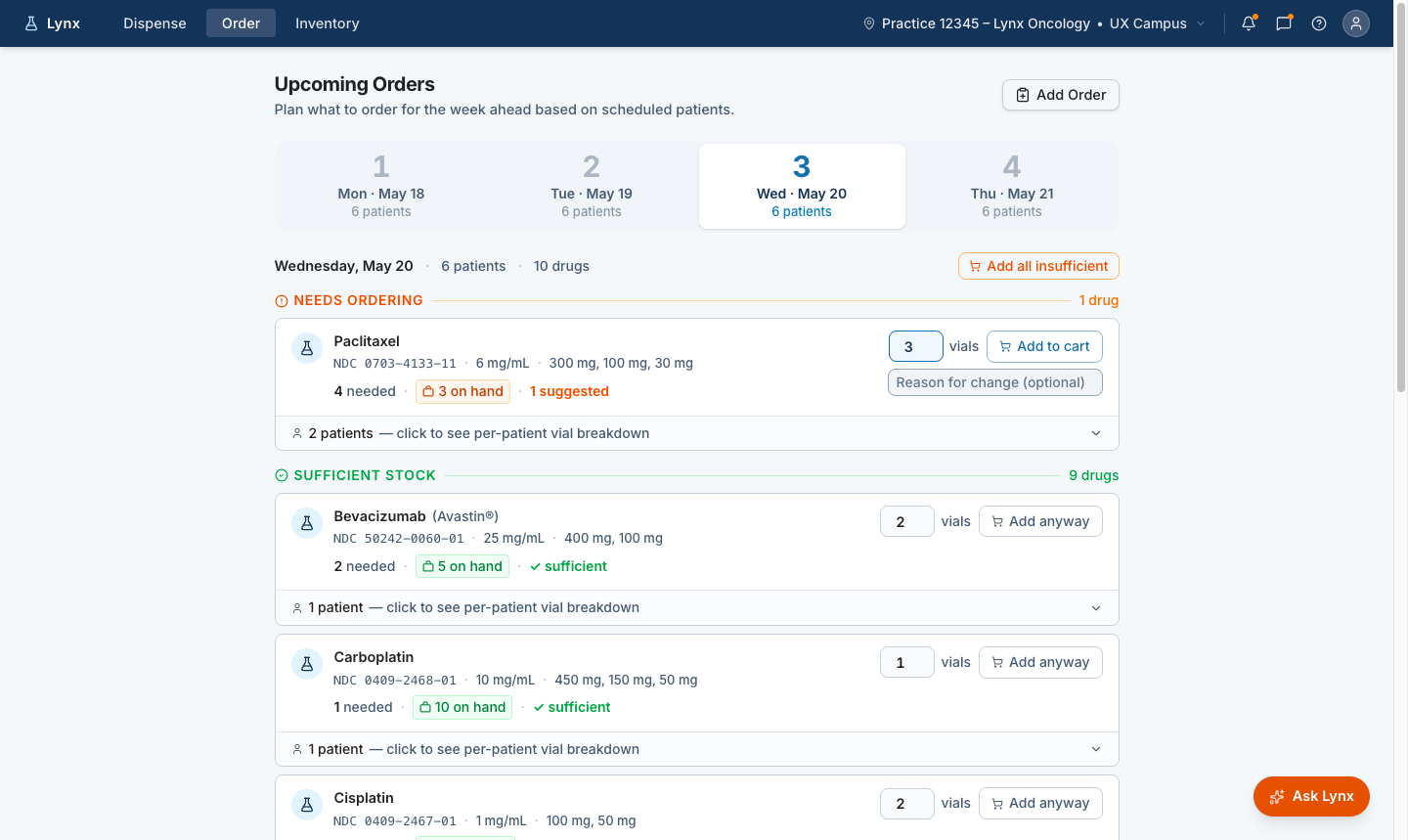
Surface medication demand before treatment day
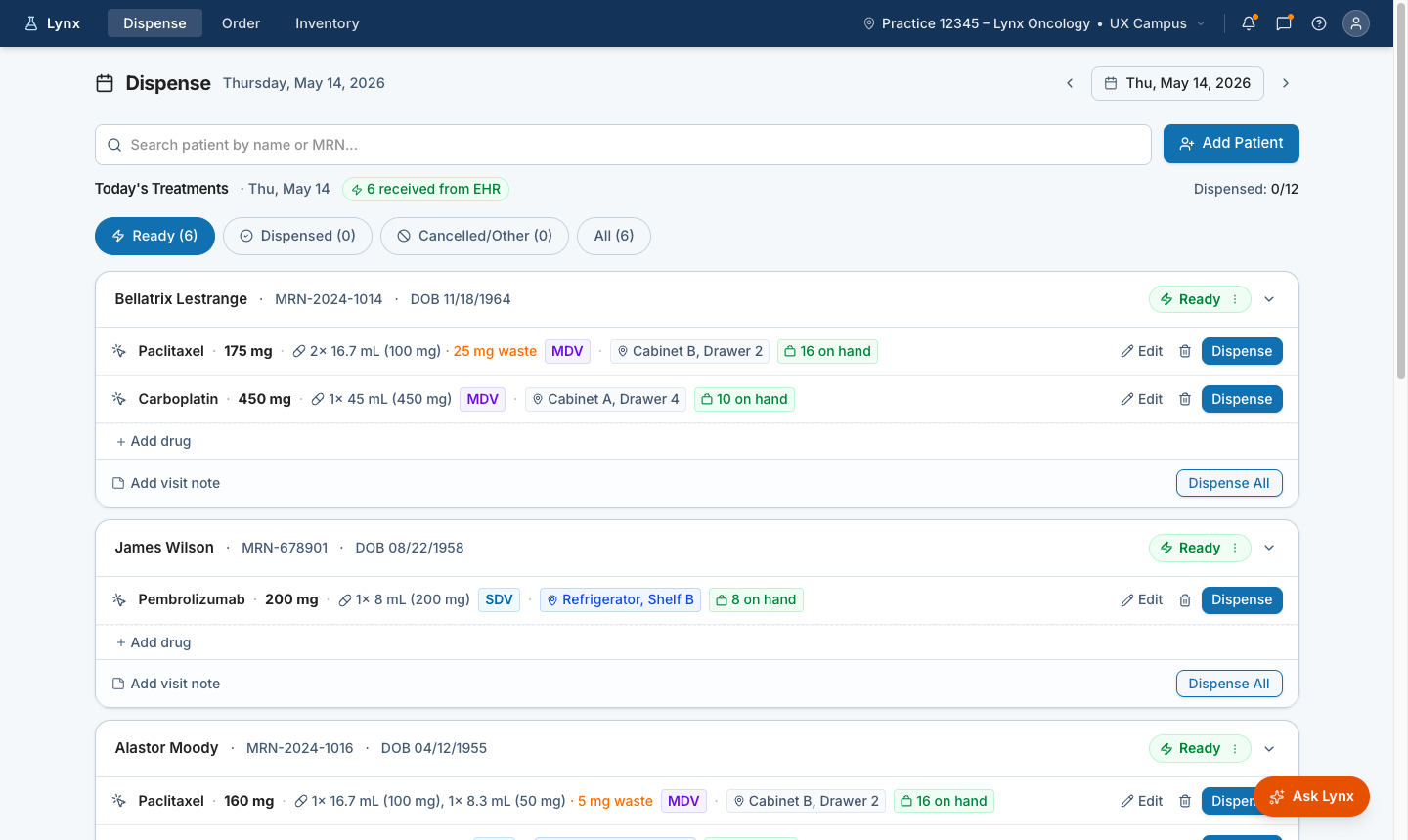
Show who is ready for dispense
Recommend vial combinations with human review
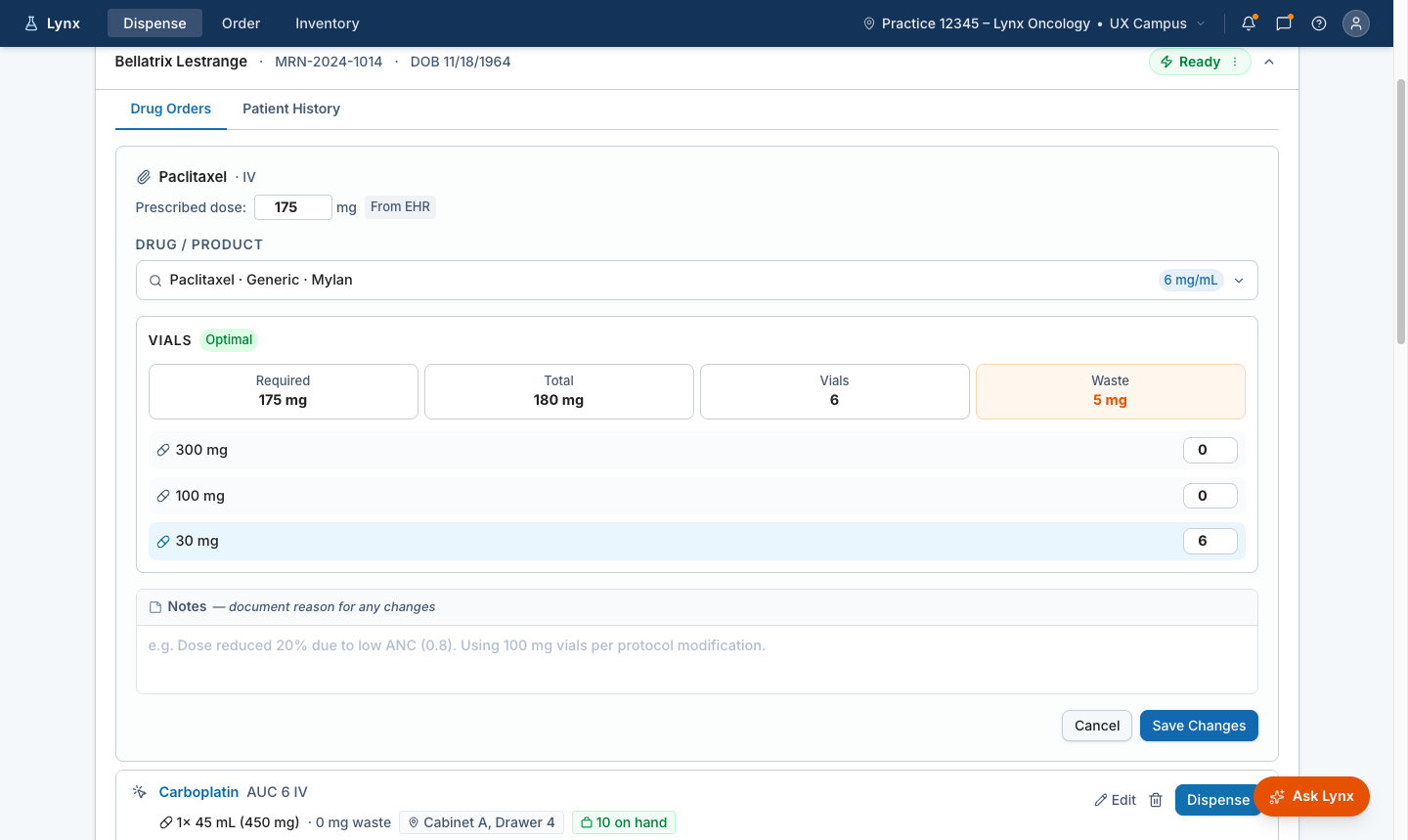
When staff adjust the recommended vial mix, Lynx recalculates waste immediately and carries the change forward with a clear adjusted state.
What this changed.
Research revealed that the queue was acting as a manual planning layer for treatment readiness. The hard work was happening before the dispense action: checking schedules, confirming clinical context, reviewing EHR updates, watching inventory, and resolving exceptions.
That shifted the product direction. We stopped designing only for the dispense moment and started designing for the readiness work that made dispensing possible.
This work later supported the AI-assisted delivery pipeline at McKesson. From design intent to production, faster →